Carpal Tunnel Syndrome: Wrist Pain and Nerve Decompression
Waking up with a tingling thumb or dropping your phone because your hand suddenly went numb isn't just annoying-it’s often the first sign of Carpal Tunnel Syndrome, a condition where the median nerve gets squeezed in the wrist. If you’ve been ignoring that "pins and needles" sensation, thinking it will go away on its own, you might be risking permanent damage. This guide breaks down exactly what is happening inside your wrist, why standard advice sometimes fails, and how nerve decompression procedures actually work to fix the problem.
You don’t need a medical degree to understand why your wrist hurts, but you do need to know when conservative treatments like splints are enough and when surgery becomes the only real option. Let’s look at the anatomy, the evidence-based treatments, and what recovery really looks like in 2026.
The Anatomy of Compression: Why Your Wrist Hurts
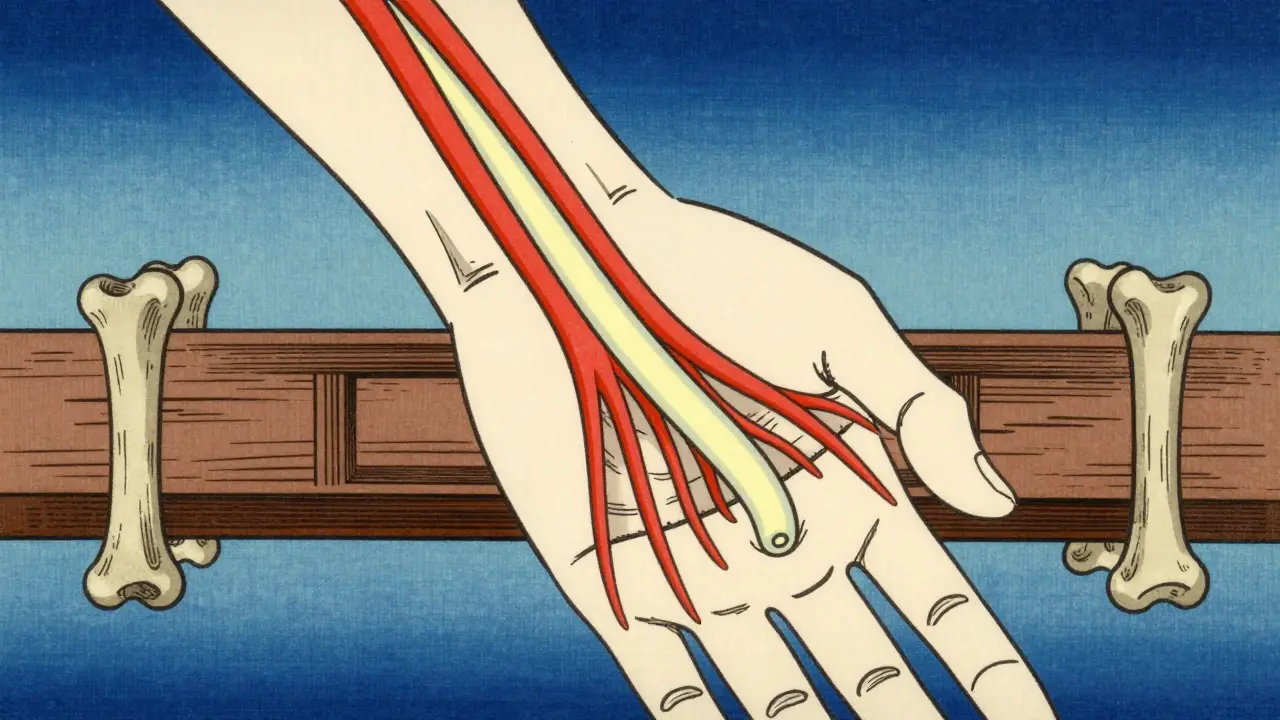
To fix the pain, you first have to understand the bottleneck. Your wrist contains a narrow passageway called the carpal tunnel. It is bounded by small carpal bones on one side and a tough band of tissue called the transverse carpal ligament on the other. Inside this tight space runs the median nerve along with nine flexor tendons.
Think of the carpal tunnel like a garden hose. The hose is the median nerve, and the surrounding structures are the water pressure. Normally, the pressure inside the tunnel is low (2-10 mmHg). But when inflammation swells the tendon sheaths or the ligament tightens, that pressure spikes-often exceeding 30 mmHg. This crushes the nerve against the bone, cutting off its blood supply and disrupting signals to your brain.
This compression specifically affects the thumb, index finger, middle finger, and half of the ring finger. If you feel numbness in your pinky, that’s usually not carpal tunnel; it’s likely a different nerve issue (ulnar nerve entrapment), so getting the diagnosis right matters.
Symptoms That Signal You Need Action
Most people dismiss early symptoms as fatigue. But CTS follows a predictable pattern. According to data from the Mayo Clinic, 50-80% of patients experience numbness and tingling in those specific fingers. The hallmark sign? Nighttime pain. About 89% of patients report waking up with shaking hands or needing to "flick" their wrists to restore feeling. This happens because we naturally bend our wrists while sleeping, which further narrows the already crowded tunnel.
If left untreated, the nerve damage progresses. You might notice:
- Thenar Atrophy: The muscle at the base of your thumb shrinks and flattens.
- Grip Strength Loss: A documented drop of 20-35% in strength, making it hard to open jars or hold tools.
- Constant Numbness: The tingling stops coming and going and becomes a permanent dull ache.
If you see muscle wasting in your thumb, time is critical. Nerves heal slowly, and once the muscle dies, regaining function is difficult regardless of treatment.
Conservative Treatments: Splinting and Injections
Before considering surgery, doctors almost always recommend trying non-invasive methods first. For mild cases-especially those lasting less than three months-conservative care works about 70% of the time. Here are the two main pillars:
Nocturnal Wrist Splinting
Wearing a brace at night keeps your wrist in a neutral position, preventing the flexion that squeezes the nerve. Research shows this can reduce symptoms by 40-60% if worn consistently for 6-8 hours nightly. The catch? Compliance. Only about 52% of patients stick with it because braces can be bulky and uncomfortable. If you try this, wear it every night for at least six weeks before judging its effectiveness.
Corticosteroid Injections
A shot of steroids into the carpal tunnel reduces inflammation quickly. About 60-70% of patients get relief for 3-6 months. However, there’s a debate here. While many clinics use injections as a first-line defense, some experts warn that repeated shots can cause tissue fibrosis (scarring), potentially making future surgery harder. Use injections as a bridge to healing or a diagnostic tool, not a permanent cure.
When Surgery Becomes Necessary
If splints and injections fail, or if you already have muscle weakness, carpal tunnel release surgery is the gold standard. The goal is simple: cut the transverse carpal ligament to expand the tunnel and relieve pressure on the median nerve. Success rates are high, with 75-90% of patients reporting significant improvement.
There are two main surgical approaches:
- Open Carpal Tunnel Release: The surgeon makes a 2-3 inch incision in the palm. This is the most common method (90% of cases) because it allows direct visualization of the nerve, reducing injury risk.
- Endoscopic Release: Uses tiny cameras and smaller incisions. Recovery is faster (mean 14 days vs. 28 days for open), but it requires specialized training and has a slightly higher risk of incomplete release if the surgeon hasn’t performed enough procedures.
Don’t let the word "surgery" scare you. It’s typically an outpatient procedure done under local anesthesia. You’ll walk out the same day.
| Treatment Method | Best For | Success Rate | Recovery Time |
|---|---|---|---|
| Wrist Splinting | Mild, intermittent symptoms | 70% (early stage) | Immediate symptom relief during wear |
| Steroid Injection | Moderate pain, short-term relief | 60-70% (3-6 months) | Days to weeks |
| Open Surgery | Severe cases, muscle weakness | 75-90% | 8-12 weeks for full strength |
| Endoscopic Surgery | Quick return to desk work | 75-90% | 2-4 weeks for light duty |
Recovery and Realistic Expectations
Surgery fixes the compression, but it doesn’t instantly fix the nerve. Nerves heal at a rate of about 1 mm per day. So, while the nighttime tingling often stops immediately after surgery, grip strength and fine motor skills take time to return.
Here’s what the timeline looks like:
- Weeks 1-2: Keep the wound dry. Move your fingers gently to prevent stiffness. Most desk workers return to work within two weeks.
- Weeks 3-4: Sutures are removed. You start gentle stretching exercises.
- Weeks 6-8: Gradual strengthening begins. Heavy lifting is still restricted.
- Months 3-6: Full recovery for manual laborers. Grip strength should normalize.
A common complaint is "pillar pain"-aching in the fleshy pads of the thumb and pinky. This happens in 15-30% of cases and is caused by scar tissue forming where the ligament was cut. It usually fades within three months but can be frustrating. Massage and anti-inflammatories help.
Risk Factors You Can Control
While genetics play a role, lifestyle factors heavily influence your risk. Women are three times more likely to develop CTS than men, partly due to smaller carpal tunnels. Obesity increases risk by 2.3-fold, so weight management is a genuine preventive strategy.
Contrary to popular belief, typing on a computer isn’t the primary culprit. A major 2023 study found no causal link between general computer use and CTS. Instead, look at forceful gripping. Jobs involving repetitive vibration (drilling), heavy lifting (>20 kg), or sustained awkward wrist positions (like dental hygiene or meatpacking) carry much higher risks. If you work in these fields, ergonomic adjustments aren’t optional-they’re essential.
Frequently Asked Questions
Does carpal tunnel surgery guarantee a cure?
Surgery has a 75-90% success rate in relieving symptoms, but it is not a 100% guarantee. Some patients may experience residual numbness or recurrent symptoms if underlying conditions like diabetes or rheumatoid arthritis are not managed. Additionally, recurrence rates are higher (45%) for those in occupations requiring repetitive forceful gripping.
How long does it take to recover from carpal tunnel release surgery?
For desk workers, returning to work takes about 2-4 weeks. For manual laborers, full recovery of grip strength can take 8-12 weeks. Immediate nighttime symptom relief is common, but complete nerve healing occurs slowly over several months.
Can I reverse carpal tunnel syndrome without surgery?
In mild cases, yes. Nocturnal splinting and activity modification can resolve symptoms in 70% of early-stage patients. Corticosteroid injections also provide temporary relief for moderate cases. However, if you have muscle weakness or constant numbness, conservative treatments are unlikely to reverse the damage, and surgery is recommended.
What causes pillar pain after surgery?
Pillar pain is aching in the thenar (thumb) and hypothenar (pinky) eminences. It results from scar tissue formation and altered biomechanics after the transverse carpal ligament is cut. It affects 15-30% of patients and typically resolves within three months with massage and anti-inflammatory medication.
Is endoscopic surgery better than open surgery?
Endoscopic surgery offers a faster initial recovery (14 days vs. 28 days) and less scar tenderness. However, long-term outcomes at 6 months are similar. Open surgery remains the gold standard because it allows direct visualization of the nerve, reducing the risk of incomplete release or nerve injury, especially for surgeons who do not perform high volumes of endoscopic cases.
Vineet Hawelia
July 15, 2026 AT 12:13It is quite illuminating to see the anatomical details laid out so clearly, particularly regarding the transverse carpal ligament. The distinction between median nerve compression and ulnar nerve issues is a vital piece of information that many patients overlook until it is too late. I appreciate the emphasis on the timeline for nerve healing, as it manages expectations realistically.
The data regarding compliance with nocturnal splinting is rather sobering. It suggests that while the medical solution is straightforward, the behavioral aspect remains the primary hurdle. One must respect the body's signals before they escalate to permanent atrophy.
Laura Odom
July 16, 2026 AT 23:28oh my gosh you guys are all so obsessed with this wrist thing lol like its not even a big deal honestly
i mean sure your hand might tingle but thats just your soul trying to escape the matrix or something right?? we are all just meat puppets dancing on strings controlled by tech giants anyway so why bother fixing the wrist when the whole system is broken??
also who cares about science facts when you can just vibe with your pain and let it be part of your aesthetic journey into darkness hahaha
Katie Caruthers
July 17, 2026 AT 00:36I simply cannot believe how many people here are ignoring the obvious moral failing in their own lives that leads to this condition. You sit there typing away, consuming content, ignoring the physical toll on your body because you are too lazy to stand up and stretch. It is selfish.
You think you are above the consequences of poor posture? No one is. And now you come here asking for sympathy when you could have prevented this by treating your body with the reverence it deserves. It makes me sick to my stomach to see such disregard for health.
Megan Crossland
July 17, 2026 AT 12:07you really should listen to your body more often instead of pushing through pain like its a badge of honor
the article says surgery is gold standard but i feel like people are scared of doctors for some reason
just get it done if its bad dont wait till your thumb muscle disappears that sounds awful
Jairam Prasad
July 17, 2026 AT 18:59Ah, the human wrist. A marvel of engineering that we proceed to dismantle with our own hands. How very ironic.
In my culture, we say that pain is a teacher, but I suppose in the West, you prefer to cut the teacher out with a scalpel. Fascinating approach. The statistics on women being three times more likely to suffer from this are telling. Perhaps it is the smaller tunnel, or perhaps it is the burden of carrying the world on shoulders that refuse to bend. Either way, the sarcasm is palpable in the air of this digital forum.
Gary Hull
July 19, 2026 AT 00:20look everyone is saying surgery is great but what about the risks?
i read somewhere that endoscopic is better but then this article says open is gold standard which is confusing af
why do doctors always want to cut stuff instead of letting nature take its course?? seems like they just want money
but whatever i guess if your hand is numb u gotta do something
Padraic Cepek
July 19, 2026 AT 04:05This is typical American healthcare nonsense. You pay thousands for a diagnosis and then another ten thousand to fix it. Meanwhile, over here, we work hard and don't complain about tingling fingers. If you can't handle a little pain, maybe you shouldn't be working in the first place. Get back to work instead of whining online about your soft wrists. Real men don't need splints.
Mildred Fierce
July 19, 2026 AT 19:21The statistical analysis presented here is fundamentally flawed in its assumption that mechanical intervention solves biological complexity. You speak of 'success rates' as if they are absolute truths, yet you ignore the systemic failure of ergonomic design in modern workplaces.
Furthermore, the emotional toll of chronic pain is dismissed entirely. You reduce human suffering to a table of percentages. It is cold. It is calculated. And it reveals a deep-seated apathy towards the individual experience of disability. We are not data points to be managed; we are complex beings whose pain cannot be quantified by a simple recovery timeline. Your arrogance is staggering.